Why do some people lose their central vision slowly over time, while others see their sight change almost overnight? And how do you know which form of macular degeneration you may be facing?
I’m Dr. Mitch Lee, Co-Owner and Principal Ophthalmologist at Eagle Eye Surgeons in Sydney. Every week, I meet patients who are worried about changes in their vision, and my role is to explain clearly what’s happening, provide the right treatment at the right time, and help people protect their independence.
Key Takeaways
- Dry macular degeneration progresses slowly, while wet macular degeneration can cause rapid vision loss.
- Early signs include blurred central vision, difficulty recognising faces, and needing brighter light for tasks.
- Smoking, poor diet, and uncontrolled blood pressure increase the risk of severe AMD.
- Anti-VEGF injections are the most effective treatment for wet AMD and can preserve sight for years.
- Regular eye exams and prompt attention to new symptoms are the best defence against irreversible damage.
Understanding Dry and Wet Macular Degeneration
Age related macular degeneration (AMD) come in two forms – what we call “dry” and “wet”.
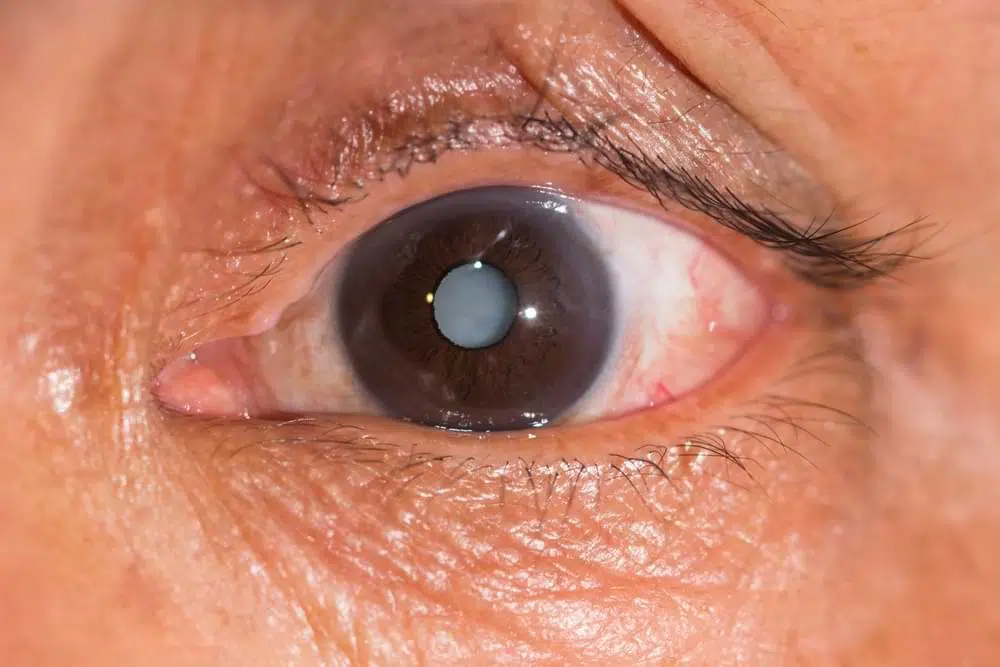
Dry macular degeneration is the quieter cousin. It begins with drusen deposits, tiny yellow specks under the retina. At first, they cause little fuss. But as they build up, they slowly rob the centre of your vision. In late stages, this becomes geographic atrophy, where patches of retinal cells stop working. It creeps along, bit by bit, often leaving you struggling with detail before you even realise.
Wet macular degeneration is more dramatic. It appears when fragile new blood vessels form under the retina, a process called neovascularisation. These vessels are like faulty plumbing that’s leaking blood or fluid that quickly damages the retina. The result is rapid vision loss, often within weeks or months if left untreated.
The key difference? Dry AMD is slow and sneaky, wet AMD is fast and aggressive. Both attack central vision, the part you rely on to read, drive, or recognise faces. Neither usually causes complete blindness, but both can change how you live your daily life.
Stages of Macular Degeneration
Which signs should you pay attention to before vision loss becomes obvious? Macular degeneration unfolds in stages, each with its own tell-tale markers.
In the early stage, most people don’t notice a thing. Vision feels normal, which is why many only discover it during a routine eye exam.
The intermediate stage brings larger drusen and subtle pigment changes in the retina. You might begin to notice a haze over fine detail or feel you need brighter light to read comfortably.
Late stage disease splits into two distinct forms. Dry macular degeneration advances gradually as the retina slowly wastes away. Central vision fades in patches, making everyday tasks harder. Wet macular degeneration moves faster, with leaking blood vessels causing sudden, severe damage. One eye can progress differently to the other, adding to the frustration.
If we recognise changes early, we can intervene, monitor closely, and protect as much vision as possible.
Symptoms and Warning Signs
Macular degeneration can creep in quietly or strike suddenly, so it’s crucial to recognize signs of condition.
- Dry AMD symptoms develop slowly. Central vision may blur, making it harder to read fine print or recognise faces. Everyday tasks often need brighter light, and detail fades gradually, as if the view is being rubbed away.
- Wet AMD progresses quickly. Straight lines may appear bent or wavy, a distortion called metamorphopsia. Dark or blank spots can suddenly block central vision, sometimes worsening within weeks if untreated. Sudden distortions should prompt a visit to an eye specialist right away.
Stay alert to these changes to preserve sight and act before damage becomes permanent.

Risk Factors and Triggers
Macular degeneration risk is shaped by both fixed traits and lifestyle choices. While you can’t change your age or family history, daily habits often make the difference in how the disease progresses.
- Age and genetics raise baseline risk. After 50, the likelihood of developing AMD rises sharply. A family history further increases vulnerability, placing some people at higher starting risk.
- Smoking and lifestyle strain the eyes. Smoking damages blood vessels and doubles the chance of severe AMD. Poor diet, uncontrolled blood pressure, high cholesterol, and long-term UV exposure all accelerate retinal damage.
- Wet AMD has additional triggers. Smoking speeds up vessel leakage, missed injection treatments allow unchecked growth, and weak cardiovascular health compounds the damage.
You can’t change age or genetics, but controlling smoking, diet, and medical conditions can slow progression and lower the risk of significant vision loss.
Diagnosis and Monitoring
We conduct our diagnosis with careful examination and the right imaging tools.
It starts with a dilated eye exam, where we look directly at the retina for drusen, pigment changes, or bleeding. We can spot subtle early signs under magnification. From there, we use optical coherence tomography (OCT). This scan works like ultrasound but uses light waves, creating cross-sectional images that reveal swelling, fluid, or thinning in microscopic detail.
We may use Fluorescein angiography if we suspect wet AMD. We inject a dye into a vein, and as it travels through the eye’s blood vessels, leaking or abnormal growth lights up on the scan. This pinpoints exactly where damage is occurring.
Patients may be given an Amsler grid, which is a simple square with straight lines, to use at home. Any new distortion or missing areas on the grid is a warning sign to book an urgent appointment.
Early and ongoing detection makes the difference between preserving sight and facing sudden, irreversible loss.
Watch the following video to learn about a simple self-test you can do at home.
Treatment Options (Anti-VEGF and Beyond)
Modern treatments for macular degeneration aim to preserve vision and, in some cases, restore clarity. Wet and dry AMD require different approaches, with current therapies focusing mainly on slowing progression and preventing further damage.
- Anti-VEGF injections are the standard for wet AMD. VEGF proteins drive the growth of abnormal blood vessels that leak and scar the retina. Targeted eye injections block this process, stopping fluid build-up and protecting central vision. The procedure is quick, done under anaesthetic drops, and with consistent treatment many patients keep functional sight for years.
- Other therapies can complement or support care. Photodynamic therapy uses a light-sensitive drug to seal leaky vessels, while laser treatments may target specific bleeding areas, though less often today. For dry AMD, no injection-based treatment exists yet, but AREDS2 supplements of vitamins and minerals can help slow intermediate disease.
- Research is pushing new frontiers. Stem cell therapy, gene therapy, long-acting drug implants, and advanced combinations are all under trial. These options hold promise for broader and longer-lasting treatment in the near future.
For now, early detection paired with consistent anti-VEGF therapy remains the strongest defence against severe vision loss.
Living With Macular Degeneration
How do you adapt when the centre of your vision no longer works reliably? The key is to take steps that protect your independence and quality of life.
Start with low vision aids. Use magnifiers, high-contrast reading lamps, and electronic devices with adjustable text to make everyday tasks easier. Train yourself in eccentric viewing—relying on healthier parts of the retina to compensate for central loss. It may feel awkward at first, but with practice, you’ll notice real improvement.
Turn everyday technology into an ally. Adjust accessibility settings on smartphones and tablets, enable voice commands, and switch to large-print displays to stay connected and entertained. Join community support groups to share experiences and remind yourself you’re not facing the condition alone.
Make lifestyle choices that strengthen your eye health. Eat a balanced diet rich in leafy greens, omega-3 fatty acids, and antioxidants to help protect your remaining retinal cells. Stay smoke-free and active to support both your eyes and your overall vascular health.
If you’d like to learn more about how to use eccentric viewing techniques to make the best use of your remaining vision, watch the following video from the Macular Society.
Frequently Asked Questions
Question: What percentage of dry macular degeneration turns to wet?
Answer: Around 10–15% of people with dry AMD will develop the wet form. This risk increases with age and advancing disease stage.
Question: Does intermediate AMD always progress?
Answer: No, not all intermediate AMD cases progress to late-stage disease. Some remain stable for years, but regular eye exams are essential to track changes.
Question: What aggravates wet macular degeneration?
Answer: Smoking, uncontrolled blood pressure, poor diet, and missing treatment appointments can all worsen outcomes. Staying on top of health and treatment plans reduces risks.
Question: How often do you need injections for wet macular degeneration?
Answer: In the first year, our patients may need injections every month or every few weeks. Once the disease stabilizes, many patients move to less frequent treatments under their ophthalmologist’s guidance.
Question: How many years does it take to go blind with macular degeneration?
Answer: AMD affects people differently, so timelines vary. Some maintain useful vision for decades with treatment, while others lose central vision more quickly, especially with untreated wet AMD. Importantly, AMD rarely causes total blindness—peripheral vision is usually preserved.
Final Thoughts
Dry AMD may move slowly, but it needs close monitoring. Wet AMD can turn lives upside down in weeks, yet today’s treatments allow many to keep reading, driving, and living independently. Know the stages, risk factors, and warning signs so you can react quickly.
You can call us on (02) 7228 3900 or arrange an appointment using the “Book Now” button in the navigation menu. We have two convenient locations: our Mosman clinic on the Lower North Shore offers ground floor access, on-site parking, and excellent public transport links; our Nepean clinic offers two hours of free on-site parking and easy access opposite Nepean Hospital.

-Ophthalmic Surgeon, Vitreoretinal, Medical Retina, Cataract, Complex Anterior Segment, Refractive and General Ophthalmology
-Fellow of the Royal Australian and New Zealand College of Ophthalmologists
-Head of Ophthalmology, Nepean Public Hospital
-Master of Medicine (Critical Care Medicine, University of Sydney)
-Bachelor of Medicine and Surgery with 1st Class Honours (University of Sydney)
-Bachelor of Science (Anatomy and Immunology, University of Sydney)
Dr Mitch is an Ophthalmologist who specialises in vitreoretinal surgery, as well as complex anterior segment, cataract, and lens surgery. He studied medicine through the University of Sydney Medical School and Royal Prince Alfred Hospital and completed his training in Ophthalmology through the Prince of Wales Hospital training network in Sydney. He is currently the Head of Department for Ophthalmology at the Nepean Public Hospital.