Why don’t some people with diabetes notice vision changes until the problem is already well-advanced?
I’m Dr Mitch Lee, Principal Ophthalmologist at Eagle Eye Surgeons, and much of my work involves helping patients protect their sight before diabetic retinopathy becomes a threat.
In clinic, we often explain that diabetic retinopathy affects almost one in three people with diabetes at some point in their lives. It can be silent for years, then shift gears quickly. My role is to detect those changes early, treat them promptly, and guide each patient with clear, practical advice that fits their lifestyle.
Key Takeaways
- Diabetic retinopathy often develops quietly, so regular eye checks are essential.
- Early diabetic retinopathy treatment for swelling or abnormal vessel growth can prevent severe vision loss.
- Blood sugar, blood pressure, and lifestyle choices influence how fast the diabetic retinopathy condition progresses.
- Modern treatments, including laser, injections, and surgery, are effective for diabetic retinopathy when timed well.
- Any rapid changes in vision should be assessed urgently.
What Is Diabetic Retinopathy and Why Does It Occur?
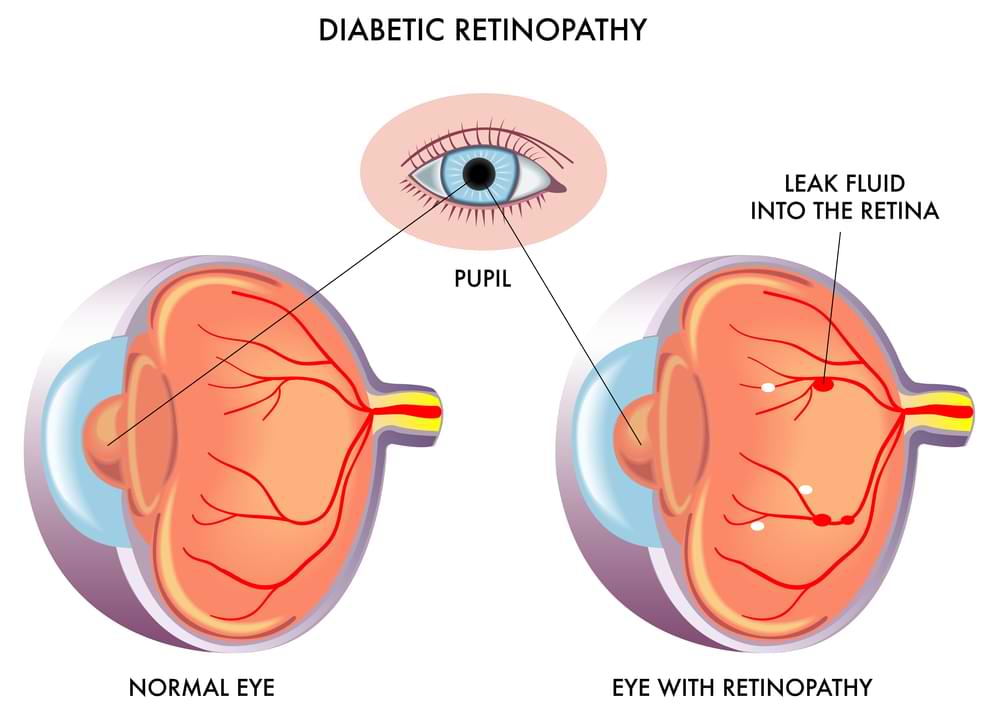
Diabetic retinopathy occurs when prolonged glucose spikes harm the tiny vessels that feed the retina. That damage develops slowly but steadily, and it places your vision at risk.
When blood sugar remains high, the smallest retinal vessels behave a bit like old plumbing under pressure. They weaken, bulge, and leak. Some close off entirely, which starves the retina of oxygen. In response, the eye tries to grow new vessels, but these are fragile and prone to bleeding. This entire cycle links directly to how well someone manages their diabetes and how closely they keep an eye on systemic health checks.
Both Type 1 and Type 2 diabetes carry a high lifetime risk of diabetic retinopathy. The longer someone has diabetes, the more likely these vascular changes are to appear, especially if glucose control drifts off track. We often describe it as a slow build-up that stays hidden until it reaches a tipping point.
What Are the Main Stages of Diabetic Retinopathy?
Diabetic retinopathy develops in three distinct stages, and understanding these stages helps patients make sense of the decisions we make during their visits.
Each phase signals a different level of stress within the retina, which is why small changes can influence how closely we review the eye over time.
- Non-proliferative retinopathy is the earliest stage and can be mild, moderate or severe. It reflects how many vessels are leaking or blocked, and how much swelling has developed. When the pattern meets the “4-2-1 rule” (severe haemorrhages in four quadrants, venous beading in two, or intraretinal microvascular abnormalities in one), we know the disease is edging closer to a more aggressive phase and requires tighter monitoring.
- Proliferative retinopathy begins when the retina becomes oxygen-starved and new vessels grow in response. These vessels are fragile and bleed easily, which can fill the eye with blood or pull on the retina. That traction increases the risk of detachment and creates a situation that needs urgent attention.
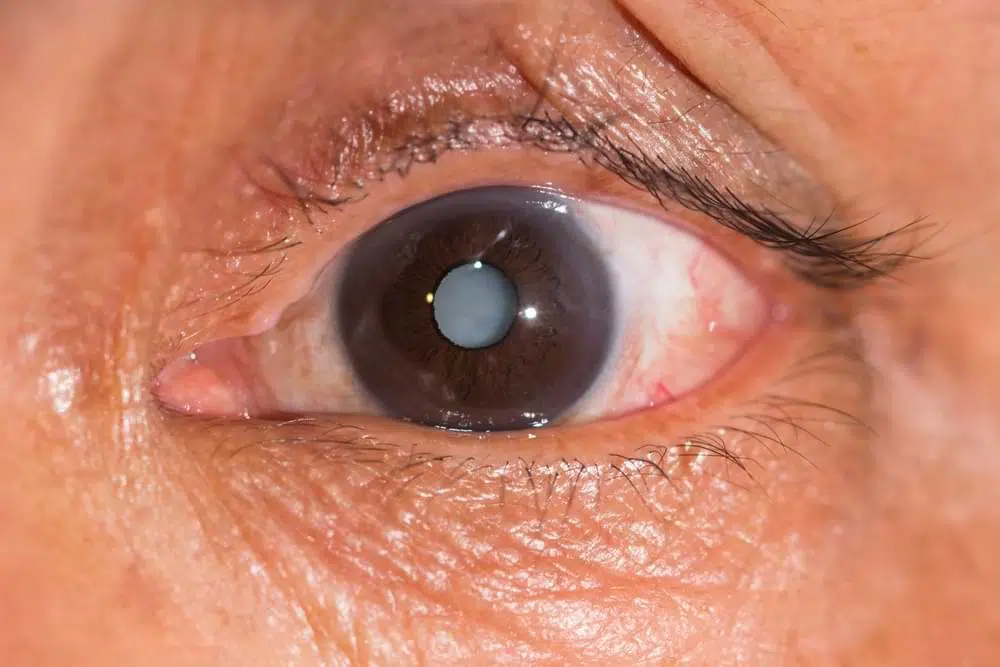
- Macular oedema can occur at any stage and directly affects central vision. Fluid leaks into the macula, causing blur, distortion and difficulty with daily tasks. It’s one of the most common reasons patients first realise something has changed.
What Symptoms Should Patients Watch For?
Most people don’t notice any symptoms early on, but as diabetic retinopathy progresses, vision changes begin to appear.
In the early stages, the retina can be quietly damaged without causing pain, redness, or any obvious warning signs — which is why routine screening is essential. As the condition advances, patients may start experiencing intermittent blurry vision, new floaters drifting across their sight, or straight lines appearing wavy or distorted.
Some patients may notice day-to-day fluctuations in vision that mirror changes in blood glucose levels. In more severe stages, when bleeding occurs inside the eye, vision can drop suddenly and dramatically, as though a dimmer switch has been turned down without warning. Regular eye examinations allow us to detect these issues long before they threaten sight.
What Systemic Factors Worsen Diabetic Retinopathy?
One of the biggest drivers of diabetic retinopathy’s fast advancement is unstable blood sugar.
When parts of the body struggle, the retina often reflects that stress, which is why we look beyond the eye when assessing risk.
- Blood sugar instability is the strongest driver of retinal damage. Wide swings or consistently high readings place constant strain on the tiniest vessels. Keeping haemoglobin A1c in a healthy range slows this process, so glucose stability remains a central part of long-term protection.
- Other medical conditions can speed progression. High blood pressure stiffens fragile vessels and increases the chance of leakage. Cholesterol problems affect circulation, and kidney disease often appears alongside more aggressive eye changes. Lifestyle habits such as smoking and poor diet compound these pressures by reducing oxygen delivery and encouraging glucose spikes.
- Pregnancy can accelerate retinopathy, especially in people with early disease. Hormonal shifts raise the pace of vessel damage, which is why we schedule more frequent reviews during pregnancy to track changes closely.
Systemic control supports retinal stability.
What Ophthalmic Treatments Are Available for Diabetic Retinopathy?
Treatment depends on the stage of disease and whether the macula is involved.
In early non-proliferative cases, our focus is often on monitoring and helping patients improve systemic control. When swelling appears in the macula or abnormal vessels develop, active treatment becomes essential to protect sight.
The aim is to steady the retina, reduce leakage, and prevent bleeding. Diabetes remains a lifelong condition, so treatment focuses on controlling the eye changes rather than removing the underlying cause. Even when vision improves, follow-up remains vital because diabetic retinopathy can shift direction without warning.
How Does Laser Photocoagulation Therapy Help?
Laser photocoagulation helps by sealing leaking vessels and reducing the signals that drive abnormal vessel growth.
- Focal/Grid Laser: Targets specific leaking areas near the macula to reduce swelling and stabilise central vision.
- Pan-Retinal Photocoagulation (PRP): Treats the wider peripheral retina to lower its oxygen demand, which causes fragile new vessels to shrink and reduces the risk of bleeding.
After treatment, mild discomfort or peripheral vision changes can occur, but these usually settle. Follow-up visits remain essential to ensure the retina is responding as expected.
How Do Anti-VEGF Injection Medications Work?
Anti-VEGF medication blocks the signals that cause swelling and fragile vessel growth.
When VEGF levels fall, the retina settles, fluid clears, and vision often improves. This is why intravitreal injections remain the gold-standard treatment for macular oedema in Australia.
We use several medications depending on the clinical picture. Eylea, Lucentis, and the newer Vabysmo are all reliable options, each with strong evidence behind them. Treatment usually begins with a run of monthly injections. Once the swelling improves, we tailor the schedule to the eye’s response so patients can maintain results with fewer visits.
Medicare covers much of the treatment, although some practices charge gap fees. We always explain the safety profile, expected outcomes and small risks before we begin. The most important part is consistency. Skipping appointments allows swelling to return, which puts vision under pressure again.
When Is Vitrectomy Surgical Procedure Required?
Vitrectomy becomes necessary when complications block clearer vision or threaten the retina itself.
A common reason is a vitreous haemorrhage that refuses to clear. When blood lingers, it acts like a curtain, leaving patients with a dark or hazy view for far too long. Tractional retinal detachment is another trigger. Scar tissue can tug on the retina with enough force to pull it out of position, and surgery is the only way to relieve that tension. Dense membranes forming on the retinal surface can also distort vision and require careful removal.
The operation involves removing the vitreous gel inside the eye through tiny incisions. Once the space is clear, we can treat underlying problems directly. Laser may be applied during the same procedure to stabilise the retina. Despite its delicate nature, the surgery is usually well tolerated.
Recovery takes patience. Vision can look cloudy for weeks before settling, and follow-up visits remain essential because the retina needs close supervision after such a significant event.
Final Thoughts
You are someone living with diabetes who wants to protect eyesight, stay independent, and avoid the stress of sudden vision changes. But you may feel uncertain about what’s happening inside your eyes, unsure whether your symptoms “matter,” and worried you’ve left things too long.
If this is you, the wisest decision is to book a consultation with Eagle Eye Surgeons today.
The main lessons are simple. Regular eye checks catch trouble early. Stable systemic health slows progression. Modern diabetic retinopathy treatments can protect your remaining sight when changes appear. And sudden vision symptoms should never be ignored.
We have two convenient locations in Sydney. Our Mosman clinic on the Lower North Shore offers ground floor access, on-site parking, and excellent public transport links. Our Nepean clinic offers two hours of free on-site parking and easy access opposite Nepean Hospital. You can call us on (02) 7228 3900 (MOSMAN) or (02) 7228 3556 (NEPEAN) or arrange an appointment online through this website.

-Ophthalmic Surgeon, Vitreoretinal, Medical Retina, Cataract, Complex Anterior Segment, Refractive and General Ophthalmology
-Fellow of the Royal Australian and New Zealand College of Ophthalmologists
-Head of Ophthalmology, Nepean Public Hospital
-Master of Medicine (Critical Care Medicine, University of Sydney)
-Bachelor of Medicine and Surgery with 1st Class Honours (University of Sydney)
-Bachelor of Science (Anatomy and Immunology, University of Sydney)
Dr Mitch is an Ophthalmologist who specialises in vitreoretinal surgery, as well as complex anterior segment, cataract, and lens surgery. He studied medicine through the University of Sydney Medical School and Royal Prince Alfred Hospital and completed his training in Ophthalmology through the Prince of Wales Hospital training network in Sydney. He is currently the Head of Department for Ophthalmology at the Nepean Public Hospital.