Ever been advised to consider a vitrectomy? Many patients come to us unsure what a vitrectomy involves, what recovery looks like, and whether it’s the right step for their situation.
I’m Dr. Mitch Lee, principal ophthalmologist at Eagle Eye Surgeons in Sydney. I perform vitrectomy procedures for patients with conditions like retinal detachment, macular holes, and significant floaters. This guide explains what vitrectomy is, the types available, why it’s done, and what you can expect before and after the procedure.
Key Takeaways
- Vitrectomy removes the vitreous gel to treat retinal problems.
- There are two main types of vitrectomy: anterior and pars plana.
- Recovery from vitrectomy usually takes 2–8 weeks.
- Risks from a vitrectomy include cataract formation, infection, and retinal detachment.
- Costs for a vitrectomy procedure vary by insurance, hospital, and procedure complexity.
What Is Vitrectomy Surgery
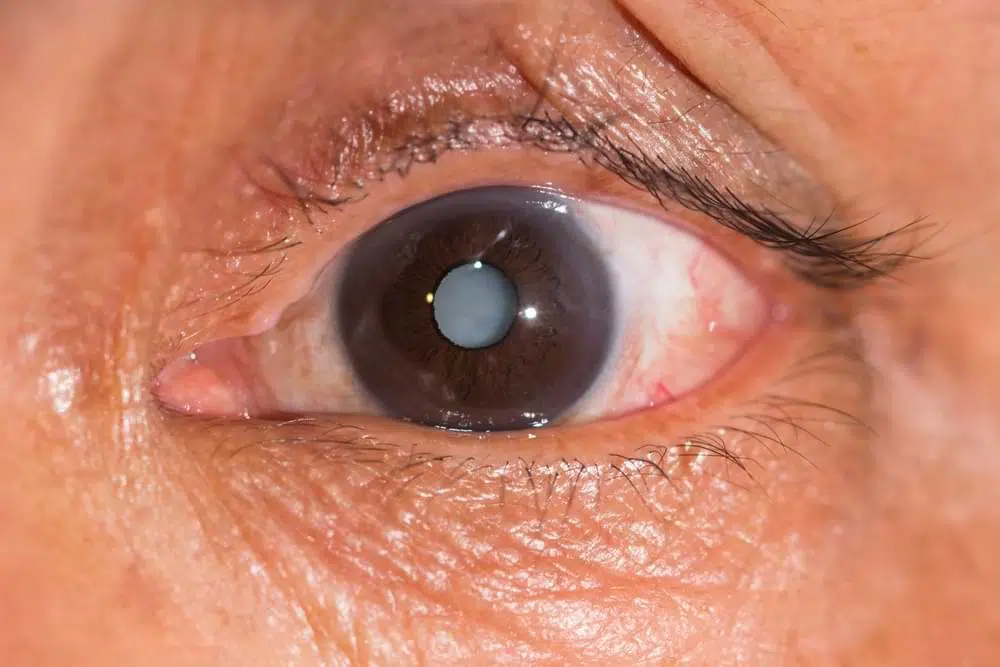
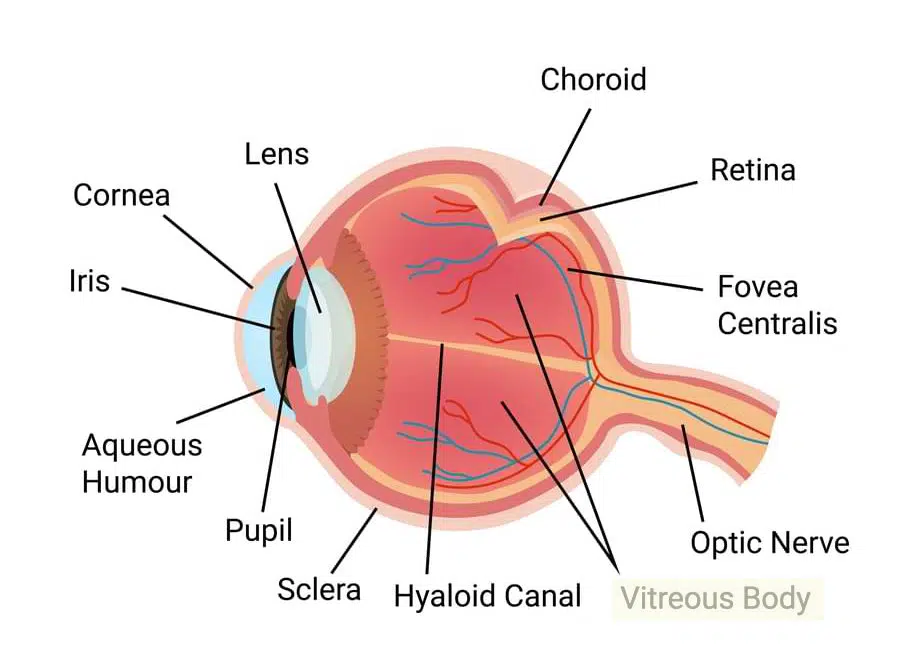
Let’s first start by defining what a vitrectomy is. Vitrectomy is the surgical removal of the vitreous humor (gel) inside the eye. This gel, while normally clear, can sometimes interfere with vision due to opacities, bleeding, or changes related to retinal disease. A vitrectomy creates the space and visibility needed to safely operate on the retina.
A vitrectomy is also the first step in repairing or treating the retina. Once the vitreous is removed, we can address problems such as tears, detachments, scar tissue, or traction pulling on the macula.
For patients with persistent floaters, a vitrectomy can remove these shadows from the visual field, restoring a clearer line of sight.
Types of Vitrectomy
There are two main approaches, determined by the condition being treated and which part of the vitreous needs to be removed.
Anterior Vitrectomy
Sometimes, during cataract surgery, the clear gel that normally fills the back of the eye (vitreous) can move forward into the front chamber. If this happens, the surgeon may perform an anterior vitrectomy. Through tiny incisions in the clear part of the eye (cornea), the displaced gel is carefully removed from the front of the eye. This procedure treats only the front portion of the gel and does not involve the retina at the back of the eye.
Pars Plana Vitrectomy
In this procedure, the surgeon places tiny, self-sealing entry ports through the white part of the eye (sclera). This allows almost all of the vitreous gel to be removed and provides direct access to the retina. Pars plana vitrectomy is the most commonly used technique for treating retinal conditions.
Pars plana vitrectomies can be done with instruments of different thicknesses, called “gauges.” A smaller gauge means a thinner, finer instrument.
| Gauge | Instrument Size | When It’s Used | Key Benefits | Limitations |
|---|---|---|---|---|
| 23-gauge | Largest of the three | Removing silicone oil, broken lens pieces, or a foreign object from inside the vitreous cavity | Strongest instruments; can handle tougher tissue and complex cases | Slightly larger incision size compared to smaller gauges |
| 25-gauge | Mid-sized | Standard choice for many vitreous and retinal procedures | Balances speed, precision, and safety; smaller incision than 23-gauge | Slightly less rigid than 23-gauge instruments |
| 27-gauge | Thinnest | Gentle, minimally invasive procedures | Smallest incisions; fastest healing; least invasive | May struggle with tougher tissue; slightly slower for large-volume removal |
Fees and Insurance Cover
In Australia, Medicare covers vitrectomy, but only at hospitals and clinics with the specialised equipment needed for the procedure. For insured private patients, out-of-pocket costs usually fall between $500 and $2,000, depending on how complex the surgery is and if other procedures are done at the same time.
What if you don’t have private insurance? In that case, costs can start around $6,000 and go over $10,000. The total depends on the length of surgery, hospital fees, and whether it’s combined with something like cataract surgery. Our team always provides a clear, itemised estimate before booking so you know exactly what to expect.
Why You Might Need Vitrectomy
Here are some of the most common reasons your ophthalmologist might recommend a vitrectomy, and how the procedure helps.
| Condition | Why Vitrectomy is Performed |
| Retinal detachment | – Repairs retinal tears and removes trapped fluid under the retina. – Places gas or silicone oil to hold the retina in position. – Early surgery improves the chances of preserving vision. |
| Macular holes | – Removes vitreous traction pulling on the retina. – Places a gas bubble to support the hole as it heals. – Can improve central vision, especially if treated early. |
| Epiretinal membrane (macular pucker) | – Carefully peels away scar tissue over the macula. – Reduces visual distortion and blurriness. – Can make reading and recognising faces clearer. |
| Persistent floaters or vitreous haemorrhage | – Clears large floaters or blood that block vision. – Allows light to pass freely to the retina. – Often used in cases linked to diabetic retinopathy or retinal tears. |
What Happens During Surgery
What’s having a vitrectomy actually like?
Before and During Treatment
In most cases, it’s done as a day procedure. You’ll have either local anaesthesia with sedation or general anaesthesia, depending on the complexity and your comfort level.
With local anaesthesia, your eye is numbed and vision is blurred, so you won’t see any instruments coming toward you.
Treatment Workflow
The surgeon makes small entry points to insert the tools. The vitreous gel is removed carefully to create a clear view of the retina. Any issues are addressed on the spot; repairing tears, removing scar tissue, or releasing traction. The entire retinal edge is checked, and any breaks found are sealed with laser or cryotherapy.
Once the retinal work is complete, we replace the vitreous with a supportive medium (air, gas, saline, or silicone oil) chosen to give the best chance of recovery.
What to Expect After Vitrectomy
Wondering how long it takes to get back to normal after post-surgery?
Day 0 – Surgery Day
- The surgeon completes the procedure under local or general anaesthetic.
- The surgical team places a protective shield over your eye.
- You rest for the remainder of the day.
Days 1–3
- You may notice mild discomfort, redness, and blurred vision.
- You start using your prescribed antibiotic and anti-inflammatory drops.
- You follow “face-down” positioning instructions if the surgeon placed a gas bubble.
Week 1
- You attend your first post-operative check-up.
- Your vision remains blurry, but gradual improvement begins.
- You avoid heavy lifting, rubbing your eye, or swimming.
Weeks 2–4
- Most discomfort subsides.
- Your vision may improve noticeably if you don’t have a gas bubble, or once it begins to dissolve.
- You continue activity restrictions as your surgeon advises.
Weeks 4–8
- Your vision keeps stabilising.
- You resume normal activities once your surgeon confirms your eye has healed enough.
- If the surgeon used silicone oil, you schedule surgery to remove it.
Months 2–6
- Your final visual outcome becomes clearer.
- You plan cataract surgery if one has developed and it affects your vision.
Risks, Complications, and Likely Outcomes
Every surgery carries some risk, but most vitrectomy patients do very well.
Typical Side Effects
- Temporary blurred vision: Common in the early recovery period as the eye adjusts and heals. Vision may gradually improve over weeks, depending on the individual.
- Cataract progression: The operated eye may develop a cataract sooner than it otherwise would. Cataract surgery can be considered later if it begins to affect vision significantly.
- Increased eye pressure: This can occur temporarily after surgery and may require short-term treatment to protect the optic nerve.
- Swelling: Some patients experience swelling inside the eye (macular oedema) which can blur vision. Anti-inflammatory medication may help reduce this.
- Bleeding: Rare, but possible during or after surgery, especially in eyes with fragile blood vessels.
- Infection: Very uncommon, but a serious complication if it occurs. Prompt treatment is needed to protect vision.
- Retinal detachment: While vitrectomy can treat detachments, there is a small risk of a new or recurrent detachment after surgery.
Success Rates & Prognosis
For many retinal conditions, reported surgical success rates are over 90%, though results vary. Visual improvement or stabilisation depends on the retina’s condition before surgery, the specific diagnosis, and how soon treatment is carried out after symptoms appear.
Scenarios Requiring Additional Surgery
Some complex cases (advanced diabetic eye disease, severe trauma, or complicated retinal detachments) may require more than one operation. Whether you need additional surgery depends on the severity of the damage, healing response, and whether new retinal problems develop during recovery.
Final Thoughts
Can vitrectomy really save vision when other treatments can’t? In many cases, yes. It’s a specialised procedure that can restore or preserve sight when conditions are too advanced for other options.
If you’ve been told to consider vitrectomy, or if you notice sudden floaters, flashes of light, or a shadow moving across your vision, it’s critical to get a thorough retinal check.
At Eagle Eye Surgeons, we guide you through every step. From diagnosis and surgical planning to post-operative care, you’ll know exactly what’s happening and what to expect at each stage.
We have two convenient locations in Sydney. Our Mosman clinic on the Lower North Shore offers ground floor access, on-site parking, and excellent public transport links. Our Nepean clinic offers two hours of free on-site parking and easy access opposite Nepean Hospital. You can call us on (02) 7228 3900 (MOSMAN) or (02) 7228 3556 (NEPEAN) or arrange an appointment online through this website.

-Ophthalmic Surgeon, Vitreoretinal, Medical Retina, Cataract, Complex Anterior Segment, Refractive and General Ophthalmology
-Fellow of the Royal Australian and New Zealand College of Ophthalmologists
-Head of Ophthalmology, Nepean Public Hospital
-Master of Medicine (Critical Care Medicine, University of Sydney)
-Bachelor of Medicine and Surgery with 1st Class Honours (University of Sydney)
-Bachelor of Science (Anatomy and Immunology, University of Sydney)
Dr Mitch is an Ophthalmologist who specialises in vitreoretinal surgery, as well as complex anterior segment, cataract, and lens surgery. He studied medicine through the University of Sydney Medical School and Royal Prince Alfred Hospital and completed his training in Ophthalmology through the Prince of Wales Hospital training network in Sydney. He is currently the Head of Department for Ophthalmology at the Nepean Public Hospital.