If you are thinking about refractive surgery, one question almost always comes up: “If I am going to develop cataracts one day anyway, why not just replace the lens now?”
It sounds logical. But eyes are not that simple.
There are three main options we are usually discussing:
- Implantable Collamer Lens (ICL)
- Refractive Lens Exchange (RLE)
- Presbyond laser treatment of your cornea
They are not competing procedures. They suit different eyes at different stages of life.
I’m Dr Erica Darian-Smith, principal ophthalmologist and surgeon at Eagle Eye Surgeons. My role is to work out which option makes sense for you now — and which one will still make sense in 10 or 20 years.
Key Takeaways
- Implantable Collamer Lens (ICL) surgery preserves your natural lens and focusing ability, making it well suited to younger patients who have not yet developed presbyopia.
- Refractive Lens Exchange (RLE) removes the natural lens and replaces it with an artificial one, and is usually more appropriate once reading vision and accommodation are lost.
- Presbyond laser reshapes the cornea while keeping the natural lens, offering an option for patients developing presbyopia who still retain some focusing ability.
- Choosing between ICL, RLE and Presbyond depends on age, remaining accommodation, prescription, corneal health and retinal risk — not a one-size-fits-all rule.
What Is the Difference Between ICL and Refractive Lens Exchange?
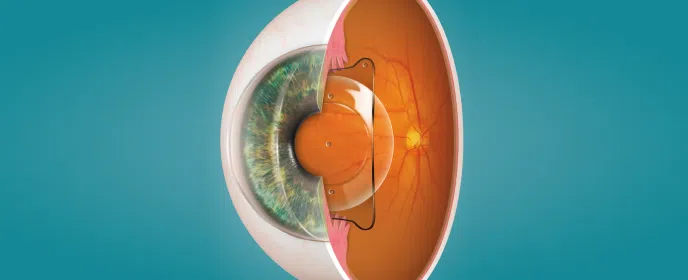
An ICL is a custom-made lens placed inside the eye. It sits behind the iris and in front of your natural lens. Your natural crystalline lens stays in place. The ICL corrects your prescription from inside the eye, much like a contact lens that lives permanently where you cannot feel it.
Refractive Lens Exchange is different. In RLE, we remove your natural lens and replace it with an artificial intraocular lens (IOL). It is essentially cataract surgery performed before a cataract forms.
That single difference — keeping or removing the natural lens — is what drives most of the decision-making.
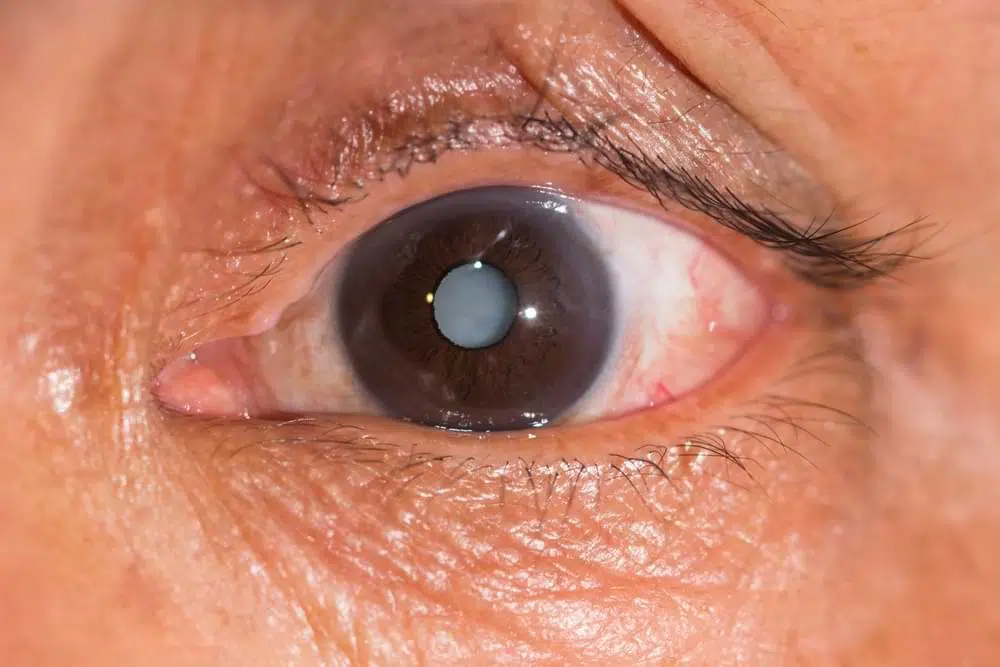
If Most People Develop Cataracts, Why Not Just Replace the Lens Early?
The answer lies in accommodation.
Accommodation is your natural lens’s ability to change shape so you can focus up close. In your twenties and thirties, that focusing system works beautifully. Even into your early forties, many people still have useful accommodation.
No artificial lens can truly replicate that natural focusing ability. Modern multifocal lenses are sophisticated and effective, but they are not the same as the lens you were born with.
If we remove a clear, functioning lens in a 35-year-old, we permanently remove that natural focusing mechanism. Once it is gone, it cannot be restored.
That is why, in general, we try to preserve the natural lens in younger patients. As a rough guide, ICL tends to suit those under about 45, while RLE is more common in patients over 50. The years in between require careful assessment. Age alone does not decide it. We measure how much accommodation you actually have left before recommending anything.
Why Do We Often Recommend ICL for Younger Patients?
For pre-presbyopic patients, ICL has some clear advantages.
For starters, it is removable if needed, which gives a degree of flexibility that lens replacement does not offer.
ICL is particularly attractive in high myopia. If you are very short-sighted, we can correct your prescription without removing any corneal tissue. The structural integrity of the cornea remains intact. This can reduce concerns around dry eye or long-term corneal stability that sometimes arise with high-prescription laser treatment.
It is also an excellent option for patients who are not suitable for laser because of thin or borderline corneas. In those cases, ICL allows us to achieve strong visual outcomes without placing stress on the cornea.
Patients often ask whether ICL interferes with future cataract surgery. It does not. If you develop a cataract later in life, the ICL can be removed at the time of cataract surgery. The lens calculations for that surgery are not compromised by the presence of the ICL.
There are some short-term visual effects after ICL, such as mild light phenomena related to the central aperture in the lens. In most cases, these settle as the eye adapts.
For a younger patient with healthy accommodation, preserving what already works well usually makes sense.
When Does Refractive Lens Exchange Become the Better Option?
RLE starts to make more sense once presbyopia is established. If you already need reading glasses and your natural lens has lost its ability to focus up close, there is less to preserve.
In that setting, removing the ageing lens and replacing it with a multifocal or extended depth of focus lens can address distance, intermediate and near vision in one procedure.
Many patients appreciate the definitiveness of RLE. Once the natural lens is replaced, you will not develop a cataract later because that lens is gone. For some people, that single-step solution is appealing.
We do, however, need to discuss side effects. Multifocal lenses can produce glare or halos, particularly at night. Modern lens designs have reduced these effects significantly, and careful patient selection is crucial. In my experience, with appropriate lens choice and good neuroadaptation, most patients cope very well.
There is also a small increase in retinal risk in certain patients, particularly high myopes without a posterior vitreous detachment. That risk varies depending on your eye’s anatomy and prescription. This is part of the pre-operative assessment and risk discussion.
RLE is permanent. That is neither good nor bad in itself. It simply means we must be confident that it is the right timing.
Where Does Presbyond Fit Between ICL and RLE?
Presbyond is a corneal laser procedure. It does not involve entering the eye and it does not remove your natural lens.
Instead, it reshapes the cornea to extend your depth of focus, creating a blended vision effect. It is often well suited to patients in their late thirties to mid-fifties who are becoming presbyopic but still retain some accommodation.
For patients who prefer to avoid intraocular surgery, Presbyond can be an appealing option. It may also be attractive to those who are particularly concerned about night-time glare associated with some multifocal intra-ocular lenses.
Presbyond does not replace ICL or RLE. It is simply another pathway depending on your visual needs and eye anatomy.
How Do We Decide Which Procedure Is Right for You?
There is no single rule that applies to everyone. We look at your eye as a whole and consider several factors at once:
- Your age and remaining accommodation
- Your prescription and degree of astigmatism
- The health and thickness of your cornea
- Your retinal risk profile
- Your occupation and night vision demands
- Whether reversibility is important to you
Sometimes two procedures are both reasonable. In those situations, we discuss the trade-offs openly. Some patients prioritise preserving their natural lens. Others prefer a definitive solution that eliminates the possibility of cataracts later.
The key point is this: we are not simply correcting a prescription for today. We are planning how your eyes will function as they age.
There is no universal “best” procedure. There is only the right procedure for your eyes at your stage of life.
Watch the following video where I explain how we make decisions with our patients about choosing a procedure together.
Final Thoughts
Choosing between ICL, lens exchange and Presbyond isn’t a black and white linear choice. Presbyond is not a compulsory “middle step” between ICL and lens replacement. Each option stands on its own. If you still have strong natural focusing ability, preserving your lens with ICL often makes sense. If that focusing system has faded, RLE may be the logical move. The key is timing and suitability — not following a predetermined sequence of procedures.
If you would like to become eyewear-free and are wondering whether ICL, RLE or Presbyond is appropriate for your eyes, then the right decision is to book a complimentary vision planning assessment with us. Often, the most important first step is simply having a clear, informed conversation about your long-term eye care needs.

– Fellow of the Royal Australian and New Zealand College of Ophthalmologists (FRANZCO)
– Fellow of World College of Refractive Surgery and Visual Sciences (FWCRS)
– GradDipGraduate Diploma in Cataract and Refractive Surgery (University of Sydney)
– Master of Medicine (MMed, Ophthalmic Sciences, University of Sydney)
– Bachelor of Medicine and Surgery (MBBS, University of Tasmania)
Dr. Erica was a recipient of the 2022 ASCRS Foundation Resident Excellence Award. In 2019, she was awarded the RANZCO Filipic Greer Medal for overall excellence in performance at the RANZCO Ophthalmic Pathology examination. Most recently, she was awarded the Royal Australian and New Zealand College of Ophthalmologists (RANZCO) Trevalyn-Smith Travelling Scholarship to subsidize overseas study for Fellows.
As an accomplished researcher Dr. Erica’s work has been published widely in high quality medical journals, including the American Journal of Ophthalmology, the Journal of Cataract and Refractive Surgery, the European Journal of Ophthalmology and Clinical and Experimental Ophthalmology. Erica has also written a book chapter and has had the opportunity to present her research at various international and national conferences. Dr. Erica is appointed as a Clinical Lecturer in the Discipline of Ophthalmology at the University of Sydney, Save Sight Institute and regularly contributes to ongoing teaching in her area of subspeciality.