What if your blurry vision isn’t just a need for stronger glasses? Could something else be quietly changing the shape of your eye?
I’m Dr Erica Darian-Smith, Principal Ophthalmologist at Eagle Eye Surgeons in Sydney. I have deep experience in diagnosing and treating keratoconus—a condition that affects thousands of Australians but is often misunderstood or missed in its early stages. My role is to help patients stabilise their vision using the latest techniques.
At my clinic, we’ve seen first-hand how timely treatment can make a lasting difference. The rise of newer methods like topography-guided corneal cross-linking (CXL) means that patients today have more effective and less invasive options than ever before. With the help of precise diagnostic tools and personalised treatment plans, many people can now avoid needing a corneal transplant altogether.
Key Takeaways
- Keratoconus causes the cornea to thin and bulge, leading to blurred or distorted vision that worsens over time.
- Corneal cross-linking can effectively stop the progression of keratoconus when caught early.
- Early diagnosis expands treatment options and reduces the need for invasive procedures like corneal transplants.
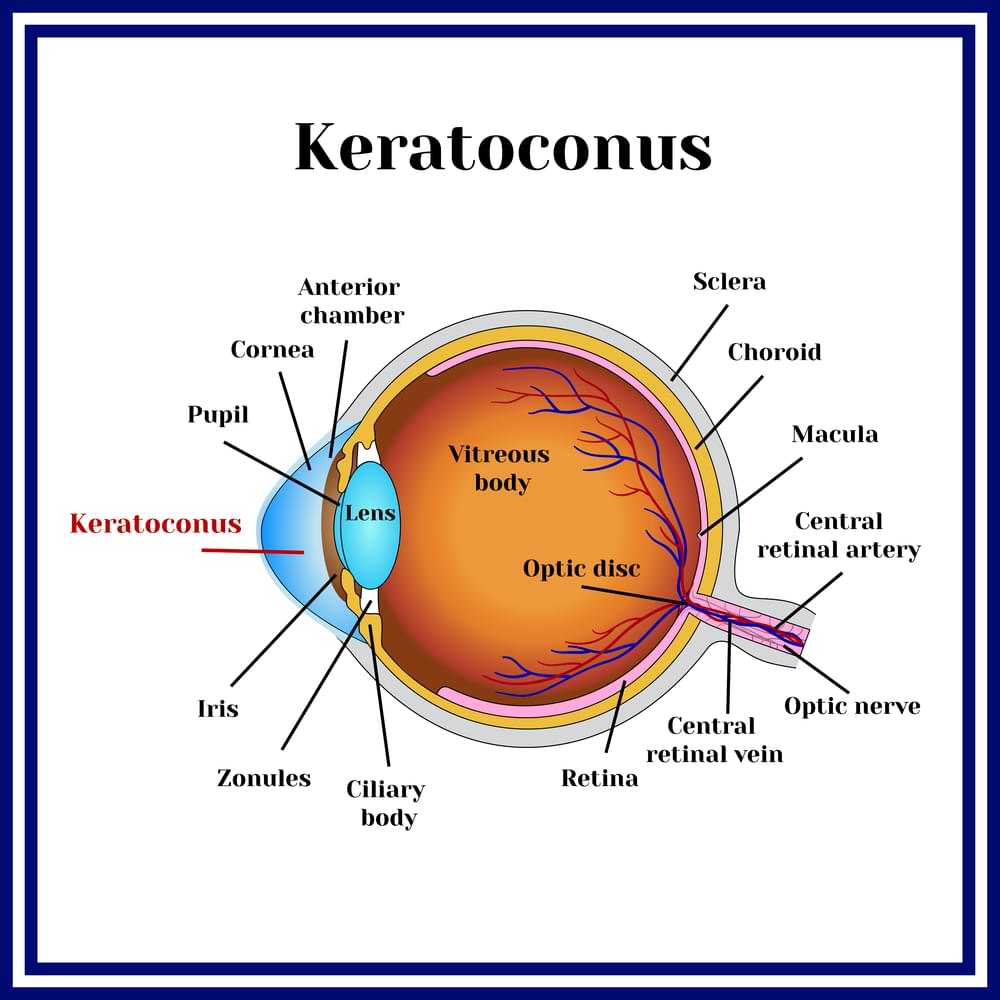
What Is Keratoconus?
Why does your vision suddenly seem blurrier, more distorted, or harder to correct with glasses than it used to be?
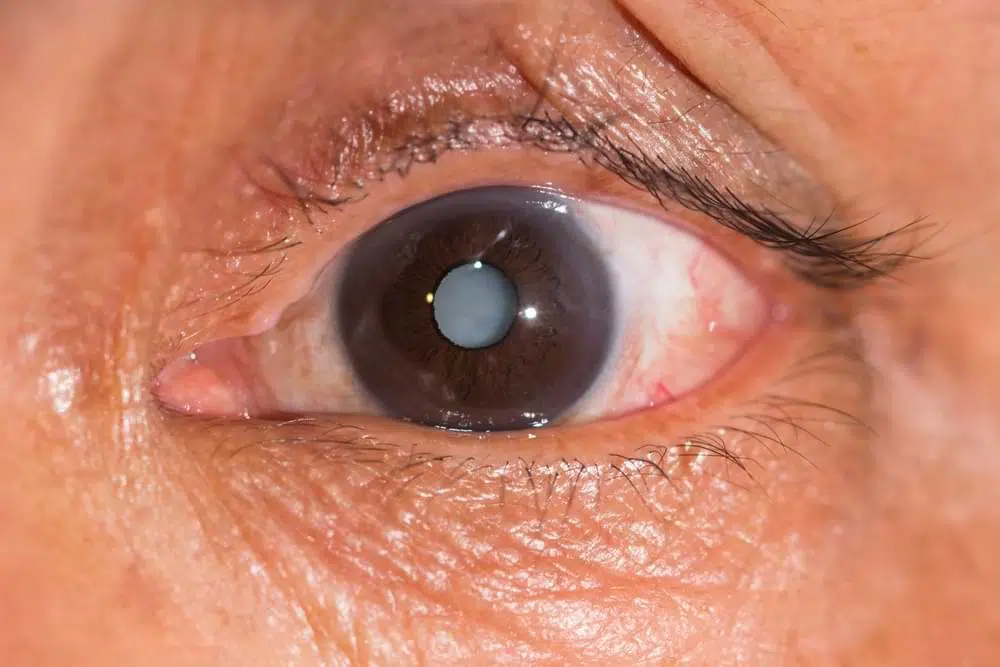
For many people, that’s how keratoconus first makes itself known. This condition causes the normally dome-shaped cornea—the clear front surface of the eye—to thin and bulge outward into a cone. When that shape warps, so does your vision. You might notice more glare from headlights at night, frequent changes to your glasses or contact lens prescription, or a sense that your eyes just aren’t cooperating the way they used to.
Keratoconus often starts in the teenage years or early adulthood. It tends to run in families and shows up more often in people of Middle Eastern and East Asian backgrounds. While rubbing your eyes might seem harmless, repeated rubbing is one of the strongest risk factors we know about. Allergies, Down syndrome, and connective tissue disorders also raise your chances.
The condition doesn’t move at the same pace for everyone. Some people have a mild case that never really causes much trouble. Others find that things get worse gradually over time. In the early stage, glasses or soft lenses may be enough. But as the cornea becomes more distorted, that’s often no longer enough to give crisp vision. At that point, we typically look at more advanced options—starting with specialty contact lenses and, if needed, surgical care.
How Keratoconus Is Diagnosed
The diagnosis starts with taking a close look at the shape and thickness of your cornea. I use a tool called a corneal topographer—it’s completely painless and works a bit like satellite mapping, but for your eye. This scan gives us a colour-coded map showing whether the cornea has started to bulge or thin, and if so, where and how much. If anything looks unusual, I’ll dig deeper.
We also check the corneal thickness with pachymetry. Thinning is one of the key signs that keratoconus might be at play. A slit-lamp exam helps me look at the cornea’s surface under high magnification, and visual acuity tests help assess the practical impact on your sight.

Overview Of Keratoconus Treatment Options
When keratoconus starts affecting your daily vision, the right treatment can make all the difference. The best treatment strategy depends on how advanced the condition is and how well your eyes respond to different forms of correction.
- Glasses and contact lenses can help in early stages. Soft lenses or updated prescriptions are often enough when the corneal distortion is mild. They provide basic visual correction without the need for invasive treatment.
- Specialty contact lenses offer sharper vision as the condition progresses. I fit patients with rigid gas permeable, hybrid, or scleral lenses depending on their needs. Scleral lenses are especially useful for irregular corneas and offer excellent comfort and clarity.
- Surgical treatment is an option for more advanced or progressing cases. Corneal collagen cross-linking (CXL) is often the first step, helping to stabilise the cornea and slow further change. For severe distortion, I may recommend intracorneal ring segments or, in advanced cases, a corneal graft.
There’s no one-size-fits-all solution for keratoconus, but there are effective tools at every stage. With the right care plan, vision can be preserved—and often improved.
Corneal Collagen Cross-Linking (CXL) Explained
Corneal collagen cross-linking is a minimally invasive treatment that strengthens the cornea using riboflavin drops (a form of vitamin B2) activated by UV light. This process creates more bonds between collagen fibres, making the cornea more rigid and less likely to bulge.
At Eagle Eye Surgeons, we offer both epi-off and epi-on cross-linking. The traditional approach, epi-off, involves gently removing the surface layer of the cornea to help the drops soak in. Epi-on leaves that layer intact, which makes for faster healing and less discomfort. I help patients choose the method that suits their lifestyle, pain tolerance, and stage of the condition.
Cross-linking works best in the early to moderate stages of keratoconus. It doesn’t reverse the shape changes, but it can freeze the condition in its tracks. The need for corneal transplants has dropped dramatically since we’ve had access to this treatment.
Understanding Intracorneal Ring Segment Surgery
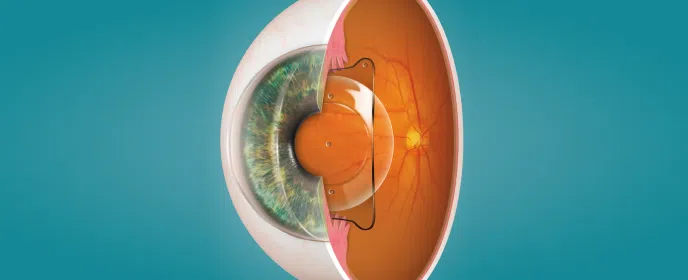
Intracorneal ring segments (ICRS) ae tiny implants, shaped like partial rings, are inserted into the cornea to help flatten and regularise its shape. This can reduce distortion and improve how light enters the eye.
There are two main types. Intacs are synthetic, while CAIRS (Corneal Allogenic Intrastromal Ring Segments) use donor tissue. CAIRS is gaining attention because it’s more biologically compatible and tends to carry fewer risks of complications. It also integrates better with your corneal structure, offering a more natural result.
ICRS can be combined with corneal cross-linking for extra stability. This pairing lets us reshape the cornea and then reinforce it to hold its new form. It’s a clever approach that avoids more invasive procedures in many cases.
Corneal Transplantation Options
For people with advanced keratoconus, corneal transplantation can be life-changing. There are two main types of grafts I use.
Deep Anterior Lamellar Keratoplasty (DALK) replaces the outer layers of the cornea but keeps the healthy inner layer intact. It reduces the risk of rejection and tends to have fewer long-term complications.
Penetrating Keratoplasty (PK), on the other hand, replaces the full thickness of the cornea and is generally reserved for the most severe cases.
Recovery from a transplant takes time and patience. There’s a longer healing period, and the risk of rejection means close follow-up is essential. But for many of my patients, a transplant gives them back clarity they haven’t had in years.
Innovations In Keratoconus Management
We’ve come a long way from one-size-fits-all treatments. Topography-guided cross-linking now lets me customise treatment patterns based on your exact corneal shape. It’s like upgrading from a standard prescription to something built specifically for your eyes.
The use of femtosecond lasers has also raised the bar. These lasers bring greater precision to procedures like ring segment placement, which translates to better outcomes and less disruption to healthy tissue.
One exciting development I use in-clinic is the Glaukos cross-linking device. It standardises treatment delivery so results are more consistent across patients. That matters when we’re aiming to prevent long-term damage and reduce the chances of needing a transplant.
And then there are combination therapies. In certain cases, I’ll pair CXL with PRK (a type of laser surface reshaping) to both stabilise the cornea and sharpen vision. Or we’ll do ring segment surgery followed by cross-linking to hold the new shape steady.
Choosing A Keratoconus Specialist in Sydney
Keratoconus requires a careful match between your stage of disease, your lifestyle, and the tools we have available. When you’re choosing a specialist, look for someone who offers both non-surgical and surgical options, not just one or the other. A clinic with advanced diagnostic equipment also makes a big difference—it helps us pick up changes early and track your progress properly.
At Eagle Eye Surgeons, we can oversee every aspect of keratoconus care—from scleral lens fitting to epithelium-on and epithelium-off corneal cross-linking. For those who need it, we also perform intracorneal ring segment procedures and corneal transplants. Our goal is always to preserve your vision for as long as possible, using the least invasive methods that will be effective.
Final Thoughts
Keratoconus doesn’t go away on its own—but we now have reliable ways to stop it in its tracks.
If your vision is changing or you’ve been diagnosed with keratoconus, I encourage you to book a consultation with us at Eagle Eye Surgeons. You’ll receive clear answers, expert care, and a treatment plan that fits both your eyes and your life.
We have two convenient locations in Sydney. Our Mosman clinic on the Lower North Shore offers ground floor access, on-site parking, and excellent public transport links. Our Nepean clinic offers two hours of free on-site parking and easy access opposite Nepean Hospital. You can call us on (02) 7228 3900 (MOSMAN) or (02) 7228 3556 (NEPEAN) or arrange an appointment online through this website.

– Fellow of the Royal Australian and New Zealand College of Ophthalmologists (FRANZCO)
– Fellow of World College of Refractive Surgery and Visual Sciences (FWCRS)
– GradDipGraduate Diploma in Cataract and Refractive Surgery (University of Sydney)
– Master of Medicine (MMed, Ophthalmic Sciences, University of Sydney)
– Bachelor of Medicine and Surgery (MBBS, University of Tasmania)
Dr. Erica was a recipient of the 2022 ASCRS Foundation Resident Excellence Award. In 2019, she was awarded the RANZCO Filipic Greer Medal for overall excellence in performance at the RANZCO Ophthalmic Pathology examination. Most recently, she was awarded the Royal Australian and New Zealand College of Ophthalmologists (RANZCO) Trevalyn-Smith Travelling Scholarship to subsidize overseas study for Fellows.
As an accomplished researcher Dr. Erica’s work has been published widely in high quality medical journals, including the American Journal of Ophthalmology, the Journal of Cataract and Refractive Surgery, the European Journal of Ophthalmology and Clinical and Experimental Ophthalmology. Erica has also written a book chapter and has had the opportunity to present her research at various international and national conferences. Dr. Erica is appointed as a Clinical Lecturer in the Discipline of Ophthalmology at the University of Sydney, Save Sight Institute and regularly contributes to ongoing teaching in her area of subspeciality.