Have you noticed that street signs look blurry at night? Or that bright sunlight on a concrete footpath leaves you squinting and disoriented? Perhaps you’ve been updating your reading glasses every six months and finding that each new pair barely helps. These experiences are more common than most people realise, and they often point to the same cause —cataracts.
I’m Dr Erica Darian-Smith, Principal Ophthalmologist at Eagle Eye Surgeons in Sydney. Alongside my colleague Dr Noor Ali, I work with patients every week who arrive unsure of what’s happening with their vision — and unsure what cataract surgery in Sydney, if it comes to that, actually involves. This article is for anyone who wants honest, detailed answers before stepping into a consultation.
KEY TAKEAWAYS
● Cataracts can be present years before they affect your vision — whether surgery is needed depends on your symptoms, not the scan alone.
● The surgery itself typically takes around 10 to 15 minutes per eye, removing the cloudy natural lens and replacing it with a precisely chosen artificial one.
● Lens selection is one of the most important decisions in the whole process, and it starts well before your day of surgery.
● Most cataract surgery patients in Sydney are back to normal life within a few weeks.
What’s Actually Happening Inside Your Eye
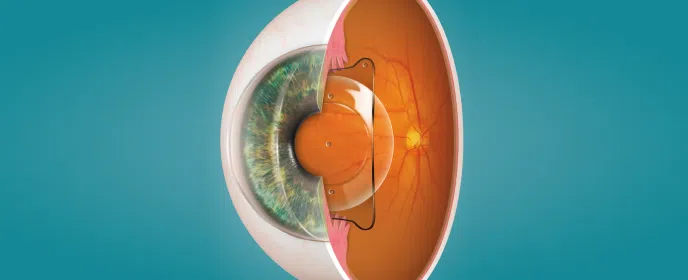
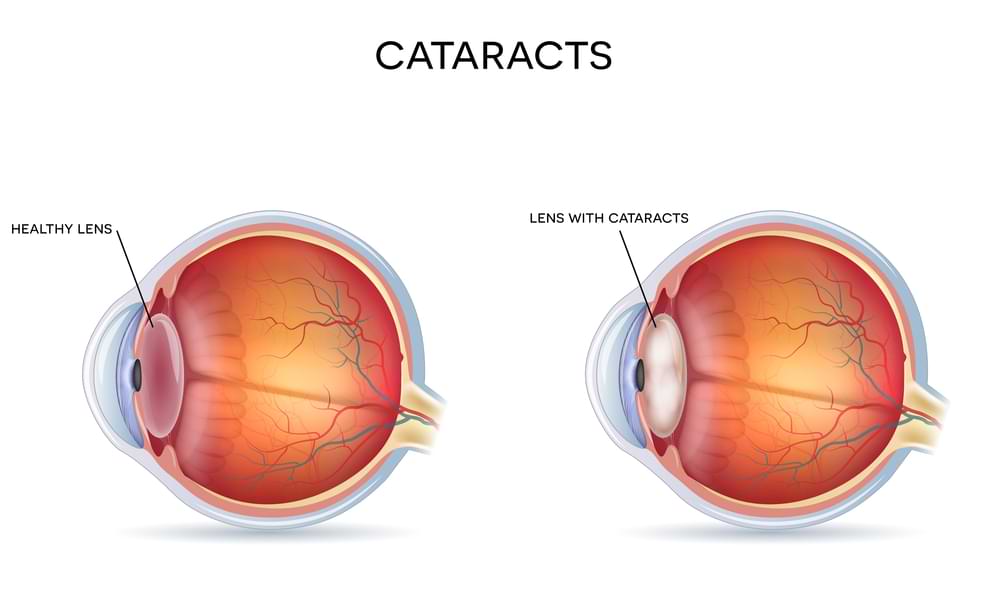
Each eye has a clear, flexible lens just behind the iris, held in place by fine fibers called zonules. From birth, this lens focuses light onto the retina — the eye’s built-in camera lens.
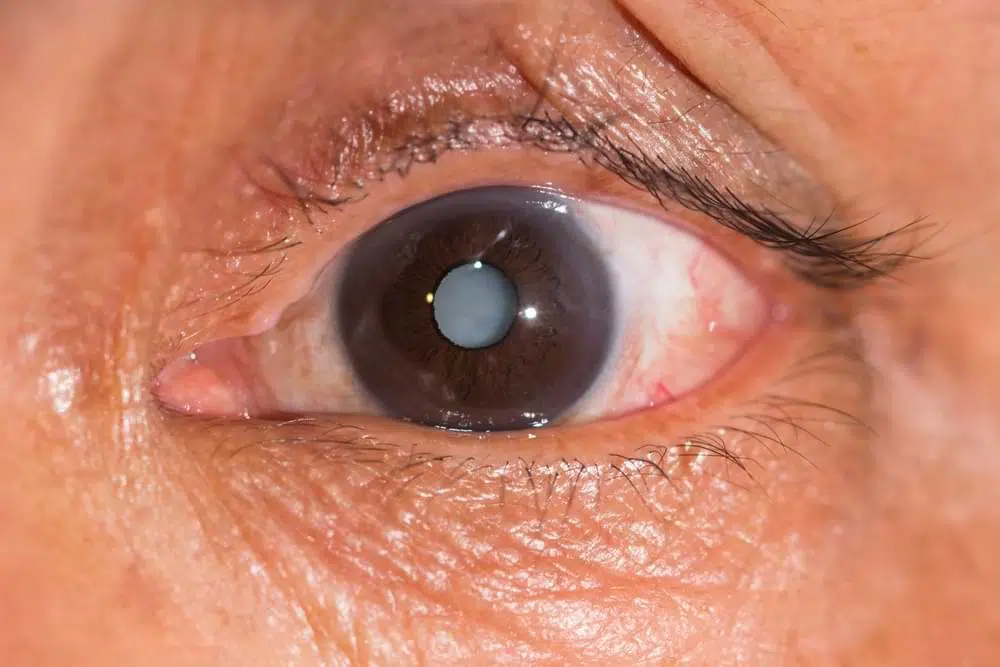
With age, its proteins break down and clump together, causing the lens to harden and cloud. That’s a cataract. The process can start at a cellular level in your 50s, though it may take decades to affect vision.
Not every cataract patient in Sydney needs surgery. The same cloudiness can affect people differently, depending on how their brain handles vision and what they do each day. A retiree reading in good light may barely notice what troubles a night driver or someone doing detailed work. The same cataract can become symptomatic at completely different times in different people.
The Symptoms That Bring Sydney Patients In For Cataract Surgery
The four most common reasons patients seek help are:
Night driving difficulties. This is often the first complaint. Patients come in with 6/6 vision at their optometrist appointment, yet describe headlights surrounded by halos and an inability to read street signs after dark. This happens because cataracts scatter light rather than focusing it cleanly on the retina.
Daytime glare. Walking on bright concrete or stepping into strong sunlight can cause significant visual impairment. The reflection of light on a pale surface hits the cloudy lens and fans out, obscuring what’s directly ahead.
Difficulty reading for sustained periods. Some patients update their reading glasses repeatedly, finding only brief relief before their vision shifts again. The underlying cause isn’t a prescription problem — it’s the lens itself continuing to change.
Not recognising familiar faces at a distance. This is one of the more socially disruptive symptoms. People find themselves unable to place a neighbour waving from across the street until they come close enough to see clearly. The loss of facial recognition at normal conversation distance can feel unsettling.
If any of these sound familiar, the right first step is a visit to your optometrist. Early cataracts can sometimes be managed with an updated prescription. But if your prescription is changing every few months, your optometrist will likely refer you on — and that’s where a surgeon’s assessment becomes useful.
Cataract Surgery Procedures In Our Sydney Hospitals
The modern cataract procedure, used in nearly all cases, is called phacoemulsification. The surgeon makes a tiny 2.2-millimetre incision, creates a circular opening in the capsule around the lens, and loosens the lens with fluid waves. An ultrasound probe then breaks the lens into small pieces, which are simultaneously vacuumed out. A folded artificial lens is inserted through the same incision and positioned inside the capsule.
Every fragment of the cloudy lens must be removed because exposed lens proteins can cause inflammation. The surgical team ensures the capsule is completely clear before placing the implant.
The operation takes about 10-15 minutes per eye under local anaesthetic with mild sedation. Most patients feel little discomfort and see improvement within a day, often noticing clearer vision within 24 hours.
The Lens Conversation: More Important Than You Think
Choosing an intraocular lens (IOL) isn’t a rushed decision, nor one you make alone. At Eagle Eye Surgeons in Sydney, we believe the art of cataract surgery lies as much in the conversation beforehand as in the procedure itself.
The process starts with your optometrist, who discusses lens options early and shares your vision history — past prescriptions, best-corrected vision, and any difference between the eyes — all of which guide lens selection.
During your surgical consultation, we ask about your work, hobbies, light sensitivity, night driving, and how much you want to rely on glasses. Lens choice influences all of these factors.
We also use an online simulator to show how each lens type affects vision, including night glare and how the brain adapts — something most patients find reassuring.
Lens options fall into three main groups: monofocal (single focus, usually distance), extended depth of focus or extended depth of focus (two distance zones), and multifocal or trifocal (near to far). Each carries trade-offs, and the best choice depends on your eyes, lifestyle, and comfort with adaptation.
To learn more about what questions your ophthalmologist will ask during the pre-surgery consultation, watch the following interview with our very own Dr Noor Ali.
What Are The Risks Of Cataract Surgery?
Cataract surgery is one of the safest and most common procedures in medicine, but no surgery is entirely risk-free.
The most serious risk is infection (endophthalmitis), occurring in about 1 in 5,000–7,000 cases, usually within the first week. Modern techniques — such as injecting antibiotics at the end of surgery, strict sterilisation, and short operating times — have made this rarer still. Patients are taught warning signs and given direct contact with their surgeon.
Technical issues, like a small tear in the capsule or a lens fragment moving backward, occur in less than 1 in 1000 cases. These may require extra procedures or a different lens choice, but with good management, most patients still regain strong vision — sometimes just more gradually.
Surgically induced astigmatism (SIA) is another small and temporary risk. With the small incision size, latest generation lens calculation formulas and the latest phacoemulsification technology this really is not a concern for our patients.
Rarer risks include macular swelling and retinal tears and detachment, all treatable if managed early.
What to Expect In The Weeks After Cataract Surgery
During the first week, we recommend wearing a protective shield during sleep and to avoid accidental rubbing. Strenuous exercise and heavy lifting should be avoided for a week, and swimming for two weeks, mainly to reduce infection risk while using steroid drops.
Most normal activities can resume quickly. Vision often returns the same day, with clarity improving over the next 24 hours and full recovery for most by four weeks.
For multifocal lenses, the brain needs time — usually less than three months — to adapt to the new range of focus. This happens naturally through everyday activities.
Whether to treat both eyes on the same day or separately depends on your lifestyle, lens choice, and any pre-existing eye issues. For multifocal users, we often treat one eye first, then assess adaptation before proceeding with the second.
Final Thoughts
Cataract surgery here in Sydney is rarely urgent — but it does deserve careful thought. Vision changes tend to creep in slowly, which makes them easy to tolerate longer than you should. But when everyday tasks start to feel harder than they used to — driving at night, reading comfortably, recognising faces — that’s usually the signal that it’s time to look deeper.
The real value of a consultation lies in understanding your options before the decision is made for you by worsening vision. If you’re noticing persistent glare, struggling with night driving, or finding that new glasses simply aren’t keeping up, then the right decision is to schedule an initial consultation with Eagle Eye Surgeons today.
We have two convenient locations in Sydney. Our Mosman clinic on the Lower North Shore offers ground floor access, on-site parking, and excellent public transport links. Our Nepean clinic offers two hours of free on-site parking and easy access opposite Nepean Hospital. You can call us on (02) 7228 3900 (MOSMAN) or (02) 7228 3556 (NEPEAN) or arrange an appointment online through this website.

– Fellow of the Royal Australian and New Zealand College of Ophthalmologists (FRANZCO)
– Fellow of World College of Refractive Surgery and Visual Sciences (FWCRS)
– GradDipGraduate Diploma in Cataract and Refractive Surgery (University of Sydney)
– Master of Medicine (MMed, Ophthalmic Sciences, University of Sydney)
– Bachelor of Medicine and Surgery (MBBS, University of Tasmania)
Dr. Erica was a recipient of the 2022 ASCRS Foundation Resident Excellence Award. In 2019, she was awarded the RANZCO Filipic Greer Medal for overall excellence in performance at the RANZCO Ophthalmic Pathology examination. Most recently, she was awarded the Royal Australian and New Zealand College of Ophthalmologists (RANZCO) Trevalyn-Smith Travelling Scholarship to subsidize overseas study for Fellows.
As an accomplished researcher Dr. Erica’s work has been published widely in high quality medical journals, including the American Journal of Ophthalmology, the Journal of Cataract and Refractive Surgery, the European Journal of Ophthalmology and Clinical and Experimental Ophthalmology. Erica has also written a book chapter and has had the opportunity to present her research at various international and national conferences. Dr. Erica is appointed as a Clinical Lecturer in the Discipline of Ophthalmology at the University of Sydney, Save Sight Institute and regularly contributes to ongoing teaching in her area of subspeciality.