Have you been told you’re not suitable for LASIK due to thin corneas or dry eyes? Or maybe your prescription is too high for laser surgery to be safe. If that’s the case, Implantable Collamer Lens (ICL) surgery might be a better option. It corrects vision without touching the cornea and can be reversed later if needed.
I’m Dr Erica Darian-Smith, refractive and corneal surgeon at Eagle Eye Surgeons. This guide breaks down what ICL eye surgery involves, who it’s suited to, and how it stacks up against other options.
Key Takeaways
- ICL eye surgery corrects high myopia and astigmatism
- It is suitable for people who are not candidates for LASIK
- The lens sits behind the iris and in front of the natural lens
- Vision usually improves within 24 to 48 hours after the procedure
- ICL avoids the dry eye risk that can follow laser-based procedures
What is ICL Eye Surgery?
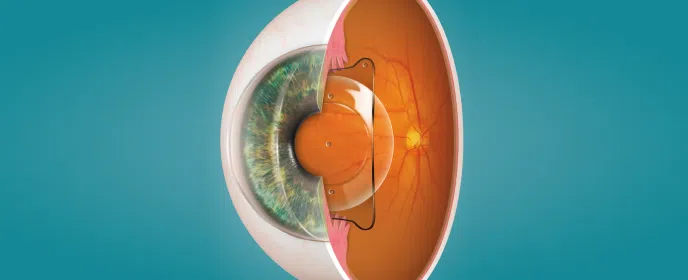
ICL stands for Implantable Collamer Lens. It’s a synthetic lens that corrects vision from the inside. Rather than reshaping your cornea with a laser, it adds a lens behind your iris. That’s why it’s called a phakic lens as it leaves your natural lens in place.
Think of it as adding a contact lens that never dries out or shifts. It stays there discreetly, improving vision, but can be removed if needed.
Is this the same as cataract surgery? Not quite. Your natural crystalline lens remains untouched.
Overview of ICL Technology
| Feature | Description |
| Lens Type | Phakic intraocular lens, preserving the natural lens |
| Position | Placed behind the iris and in front of the crystalline lens |
| Material | Collamer: a soft, biocompatible blend of polymer and collagen |
| UV Protection | Built-in UV blocker supports long-term retinal health |
| Central Port | Allows natural fluid flow, avoids need for iridotomy |
| Visibility and Comfort | Invisible to the naked eye, cannot be felt once implanted |
| Manufacturer | STAAR Surgical, Switzerland |
| Structural Advantage | Avoids corneal thinning and maintains biomechanical integrity |
Who is a Suitable Candidate for ICL?
How do you know if you’re fit for ICL eye surgery? A good ICL candidate is aged 21 to 45, has had a stable prescription for at least a year, and is looking to get out of glasses or contacts. They often have high myopia, significant astigmatism, or corneas too thin for safe laser reshaping.
It also suits people with chronic dry eye, where LASIK could potentially worsen symptoms. If laser options have been ruled out, ICL keeps correction on the table.
In the end, you keep your natural lens. You avoid corneal disruption. You get the permanent correction with the flexibility of reversibility.
Contraindications and Cautions
As with many forms of eye treatment, ICL surgery is not ideal for everyone. The following conditions may rule it out:
- Cataracts or signs of lens opacity
- History of glaucoma or uncontrolled eye pressure
- Anterior chamber depth less than 3.00 mm
- Active eye infection or inflammation
- Unstable vision prescription
- Low endothelial cell count, based on age-adjusted minimums
During your consultation at Eagle Eye Surgeons, we conduct a full ophthalmic workup to check for these risk factors before recommending any procedure.
Key Benefits of ICL Eye Surgery
Visual outcomes and reversibility
ICL provides clear, high-definition vision, especially in low light conditions. The lens can be removed or exchanged in future if prescriptions change.
Comfort and eye health
ICL has a lower impact on tear film compared to laser surgery. It avoids disturbing corneal nerves, reducing the chance of post-operative dry eye symptoms.
UV protection and long-term safety
The lens includes a built-in UV filter to support long-term retinal health. Because no tissue is removed, the procedure keeps the eye’s natural focus mechanism intact.
What Happens During the ICL Procedure?
Pre-op assessment is precise. We check corneal thickness, anterior chamber depth, endothelial cell count, pupil size, and your overall eye health. Based on these metrics, custom ICL lenses are ordered. STAAR Surgical makes them to spec.
Surgery day is straightforward.
- You’ll get local anaesthetic drops and mild sedation.
- A micro-incision is made.
- The lens is folded, inserted, and allowed to unfold into position behind the iris.
How long does the procedure take? Generally, one eye takes around 10 to 15 minutes. We usually operate on both eyes the same day under general anaesthetic.
Post surgery, you may feel some irritation or light sensitivity. That settles quickly. Most people see clearly within 24 to 48 hours. You’ll be on a short course of eye drops. Most return to normal activity within a week.

Understanding the Risks and Limitations
Like any procedure, ICL eye surgery comes with some risk. Night halos, glare, or lens decentration can occur. Pressure buildup is rare but possible. In highly myopic eyes, retinal detachment risk remains present, regardless of procedure type.
Follow-up care is necessary for proper monitoring. We monitor intraocular pressure, lens placement, and overall function. Catching issues early is the key to long-term outcomes.
Comparing ICL to LASIK and Other Options
| Aspect | ICL | LASIK | PRK |
| Procedure Type | Lens implant behind iris | Corneal reshaping with a “flap based” surgical procedure | Corneal reshaping with a “cornea surface” procedure |
| Tissue Removal | No | Yes | Yes |
| Suitable For | High myopia, thin corneas, dry eyes | Mild to moderate refractive errors | Thin or irregular corneas |
| Reversibility | Yes | No | Varies |
| Dry Eye Risk | Very low | Higher | Varies |
Choosing an ICL Surgeon in Sydney
You want a surgeon with experience beyond general eye surgery, but specifically with phakic lenses. Look for someone who understands the nuances, has a record of strong surgical outcomes, and offers proper follow-up.
At Eagle Eye Surgeons, we offer end-to-end care.
That includes diagnostics, surgery, and long-term monitoring. During your consult, we look at your prescription stability, eye health, and your goals. From there, we work out if ICL is the right fit or if something else would work better.
Final Thoughts
ICL eye surgery offers a safe and effective option for people who are not suitable for LASIK or PRK. It provides high-definition vision, avoids corneal disruption, and is reversible if your needs change. If you have been turned down for laser surgery or want a longer-term solution with fewer dry eye issues, ICL could be the right choice.
We have two convenient locations in Sydney. Our Mosman clinic on the Lower North Shore offers ground floor access, on-site parking, and excellent public transport links. Our Nepean clinic offers two hours of free on-site parking and easy access opposite Nepean Hospital. You can call us on (02) 7228 3900 (MOSMAN) or (02) 7228 3556 (NEPEAN) or arrange an appointment online through this website.

– Fellow of the Royal Australian and New Zealand College of Ophthalmologists (FRANZCO)
– Fellow of World College of Refractive Surgery and Visual Sciences (FWCRS)
– GradDipGraduate Diploma in Cataract and Refractive Surgery (University of Sydney)
– Master of Medicine (MMed, Ophthalmic Sciences, University of Sydney)
– Bachelor of Medicine and Surgery (MBBS, University of Tasmania)
Dr. Erica was a recipient of the 2022 ASCRS Foundation Resident Excellence Award. In 2019, she was awarded the RANZCO Filipic Greer Medal for overall excellence in performance at the RANZCO Ophthalmic Pathology examination. Most recently, she was awarded the Royal Australian and New Zealand College of Ophthalmologists (RANZCO) Trevalyn-Smith Travelling Scholarship to subsidize overseas study for Fellows.
As an accomplished researcher Dr. Erica’s work has been published widely in high quality medical journals, including the American Journal of Ophthalmology, the Journal of Cataract and Refractive Surgery, the European Journal of Ophthalmology and Clinical and Experimental Ophthalmology. Erica has also written a book chapter and has had the opportunity to present her research at various international and national conferences. Dr. Erica is appointed as a Clinical Lecturer in the Discipline of Ophthalmology at the University of Sydney, Save Sight Institute and regularly contributes to ongoing teaching in her area of subspeciality.