At Eagle Eye Surgeons, we are proud to offer a comprehensive range of eye procedures, including eyelid surgery for both functional and cosmetic concerns. Upper eyelid conditions such as hooded eyelids and ptosis can affect not only appearance but also vision and daily activities. For this reason, careful assessment and appropriate surgical management are important.
We are delighted that Dr Freny Kalapesi, an experienced oculoplastic and ophthalmic surgeon, has recently joined our team. Dr Kalapesi has specialist training in eyelid, lacrimal and orbital surgery and completed advanced oculoplastic fellowship training in the United Kingdom, in addition to holding a PhD in ophthalmic research. She has extensive experience managing eyelid conditions including ptosis, blepharoplasty, eyelid malpositions, watery eyes and orbital disease.
In this article, Dr Kalapesi explains the difference between hooded eyelids and ptosis, how we assess these conditions, and the surgical options available.
Upper Eyelid Surgery
By Dr Freny Kalapesi
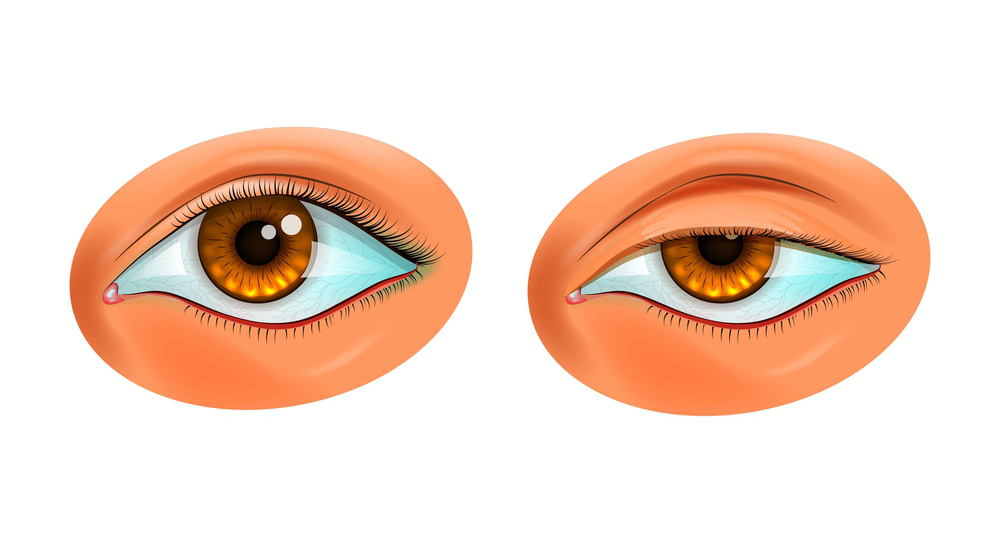
Hooded Eyelids or Ptosis: What’s the Difference and How Can You Tell?
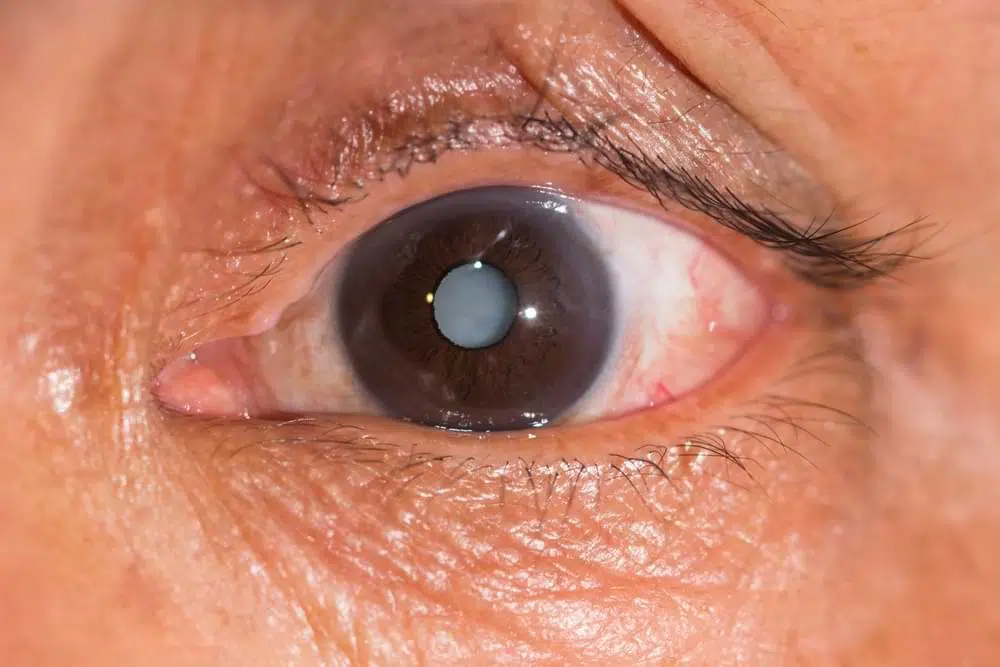
Many people notice their upper eyelids becoming heavier or lower over time, leading to a tired, aged, or asymmetric appearance. Not all eyelid drooping is the same. There’s an important distinction between hooded eyelids (dermatochalasis) and dropped eyelids, ptosis (pronounced “toe-sis”) from the Greek word meaning dropped or fall although they commonly co-exist.
Why do people seek out upper eyelid surgery
Some seek surgery for appearance concerns- they don’t like the way they look, or they can no longer wear makeup as it smudges and smears, some want to change the way their upper eyelids look, for example create an upper eyelid crease (or double eyelid) but for some the problem is much more functional with the upper lids hindering superior visual field and if severe, vision altogether, limiting function and creating evening tension headaches.
Earlier on patients feel okay during the day, and later on in the day or evening when they are fatigued and less likely to be using their frontalis muscle in their forehead, they feel their upper lid heaviness becomes more cumbersome or noticeable. On occasions, patients can be observed to use a head tilt or lift their chin to see beyond their droopy upper eyelid interfering with daily activities such as reading or driving.
What causes the appearance of heavy eyelids
Heavy eyelids could be due to mechanical causes such as low brow position, heavy excessive skin or prolapsed, prominent orbital fat pads, eyelid lesions splinting the eyelid down or ptosis ( a weakened levator or mullers muscle, muscles which are involved in opening the eyelid or looking up with the eyelid). There are a variety of causes of ptosis.
Causes of Ptosis
- Aponeurotic
● The most common type
● The levator muscle may be weakened due to common causes such as ageing, contact lens repetitive use causing stretch and eye-rubbing.
Repetitive eye surgery, and use of a rigid speculum at the time of surgery can be a frequent cause in patients who may have had glaucoma, cataract and retinal surgery - Congenital
● Tend to need different surgical repair due to poor levator aponeurosis muscle which is abnormal in it’s appearance and function.
Untreated this can lead to amblyopia (or visual deprivation, lazy eye) which can be not reversed in adulthood - Mechanical
● Skin excess, brow ptosis (or brow descent), retained foreign body under an eyelid, lesions or tumours, swelling/ scarring. These days fillers can be a mechanical cause could be a myogenic cause). Swelling can also be present from allergy or floppy eyelid syndrome associated with obstructive sleep apnoea. - Myogenic
● Including myasthenia gravis, myotonic dystrophy, CPEO - Neurological
● Can include IIIrd nerve palsies and Horner’s disease - Masquerader- Pseudo ptosis
● Contralateral eyelid retraction (eg from Graves disease), or vertical globe misalignment (known as a dystopia)- for eg. due to a tumour or inflammatory mass
How we assess eyelid patients?
History
● It is important to know the duration, speed of onset, and if there is any variability. Aponeurotic ptosis tends to be worse during the day. Myasthenia gravis may fluctuate with ptosis present at some times and absent others, or even the presence of intermittent or gaze evoked diplopia.
● Enquiry about the use of contact lens, eye rubbing or previous eye surgery especially if multiple surgeries which can stretch the upperlid levator aponeurosis muscle. A history of atopy or sleep apnoea which can cause inflammation under the eyelid.
● For a child, a history of trauma or sudden onset, may lead to a finding of a finding of a buried broken pencil lead or other foreign body or even reveal an unknown penetrating eye injury.
● It is important to know what the patient is looking to achieve, they may hold up their eyebrows or pinch their upper eyelid skin. This shows the surgeon what they are hoping to achieve. They may be seeking a procedure which an upper eyelid blepharoplasty may not achieve but a brow lift or ptosis may.
● It is important to enquire regarding symptoms- they may say they feel heavy, or have a hooded feeling. They may see their lashes or skin in their vision or feel they can see more if they lift their brows or skin manually. They may describe irritation due to skin on skin rub. They may complain they look more tired than they used to or ‘everyone thinks I’m tired when I’m not’.
I always now enquire regarding a history of recent ‘facial injectables’ – what and when. Botulinum toxin can be used to both prevent forehead rhytides and movements and consequently make the brows descend. They can also be used in the aesthetic world near the eyebrows, often near the lateral 1/3 to paralyse the orbicularis oculi (the muscle contributing the eye closure), consequently causing a relative win for the elevator of the brow, causing a chemical brow lift. Without knowledge of these treatments, decisions made by the surgeon can consequently mean too much or too little skin may be removed if this toxin is at play at the time of assessment and surgery.
As with all surgeries it is important to know about medications including blood thinners, supplemental medications which can affect bleeding time. Particularly in the case of ptosis, which shortens the levator muscle, asymmetrical bruising and significant bleeding can hinder intraoperative decisions regarding setting of the eyelid height. Ptosis surgery is often performed with an awake very lightly sedated patient such that intraoperative eyelid height titration can occur.
● A past ocular history such as dry eye, VII nerve palsy, glaucoma filtering surgery or corneal graft surgery, would mean more conservative surgery especially in cases of ptosis repair, to prevent ocular surface exposure and worsening dry eye (risk of corneal ulcers, secondary keratitis or corneal perforations) or exposing a filtering glaucoma bleb and risking endophthalmitis (serious blinding eye infection).
Examination
Examination includes examining to exclude conditions such as myasthenia gravis, CPEO, III nerve palsy or Horner’s in the case of ptosis, as well as examining protective reflexes or any ocular conditions necessitating cautious surgery (for a cornea or globe at risk- listed above in history). Examination and discussion regarding skin crease positioning can be important and is unique to a person, as this can affect the cosmesis or look a patient achieves and may change their appearance in a way that makes them look different to how they looked in their youth. Examination of the brow position is also important to determine if brow lifts or stabilisation surgery should be combined. Fat pad prominence or hollowness (deep uppereyelid sulci) are noted, as this can be addressed by addressing the fat of the orbits at the time of surgery. Often a ptosis may appear one sided, but lifting this reveals the other side is also ptotic but being masked due to a tricky physiological condition known as Herring’s law of equal innervation (if you feel like doing some googling). Thus, usually ptosis surgery is performed bilaterally even in patients often presents with what looks like a unilateral ptosis.
The extent of the upper eyelid excursion between up and downgaze (levator function) determines the surgical choice for correcting the ptosis. Poor levator function precludes routine levator recession surgery. Examination needs to exclude red flag conditions also.
Examination
- Observe: for a dystopia/ mass of orbit/ eyebrow position/ is the other eyelid high/ lifting the ptotic eyelid to observe the other eyelid
Fat pad prominence, or deep upper eyelid sulci (hollowness) - Measurements including
MRD1 (marginal reflex distance or distance from the upper eyelid margin to the corneal light reflex whilst the brow is stabilised and hooded skin is lifted to reveal the upper eyelid margin), levator function and skin crease.
- Measure for dystopia or proptosis
- Pupils, Motility and examining for upgaze fatiguability or diplopia
● Exclude horners, IIIrd nerve palsy (aneurysm potentially) or myasthenia gravis - Protective mechanisms- inability to close eyes fully on gentle closure (lagophthalmos), orbicularis muscle function and Bell’s reflex (the upward movement of the eye on closure, protecting the cornea from exposure)
- Slit lamp exam including eyelid eversion to exclude eyelid inflammation, retained foreign body, or an entry wound for a penetrating eye injury as well as examining the anterior and posterior segment of the eye. Some conditions may limit surgical intervention, and others may point to an unusual causes of ptosis.
MBS item number and AHPRA
Medicare item number reimbursement for blepharoplasty is limited to functional impact with vision impact or intertriginous inflammation of facial asymmetry. Documentation with photography and visual fields is suggested. Ptosis is easier to access MBS item number reimbursement.
More recently AHPRA has defined criteria for medical practitioners who perform cosmetic surgery including blepharoplasty surgery to try to safeguard patients following an increasing number of reported incidents in the sphere of cosmetic doctors not belonging to s surgical college body. These guidelines include that patients must have surgery by a surgeon, in an accredited surgical facility, have 2 preoperative consults, be screened for body dysmorphic disorder and be referred appropriately if concerns arise. The link to the guidelines can be found at the tail of this article.
Surgery
Blepharoplasty surgery addresses reshaping the eyelids without altering the resting position of the eyelids on the globe. Typically surgery involves reduction of excess skin folds, positioning skin creases, and reducing or repositioning fat prominences in the eyelids.
In some patients blepharoplasty alone, may not achieve what is required. Ptosis surgery and blepharoplasty can occur concurrently, and in some instances brow surgery can also occur separately or concurrently.
Risks of Surgery and Postoperative care
Severe risks are rare. Risks include excessive bleeding, swelling, scar, underdoing skin reduction (all skin is removed keeping in mind protection of the eyes), over-correction, dehiscence of wounds, asymmetry, wound infections and the need for further surgery. Most surgery is routine but postoperative bruising, swelling, scar and initial lid margin numbness is to be expected. Lagophthalmos, can occur initially with swelling. Postoperative patients should apply regular preservative free lubricant eye drops and gels as well as frequent ice packs to their eyelids, avoid strenuous activity, eyelid makeup and contact lens wear.
The full cosmetic and functional results may not be apparent for up to three months after surgery.
Timing of Surgery
Surgery should be undertaken before cataract surgery if ptosis is significant as upper eyelid position can alter corneal curvature, and on occasions change refractive outcomes achieved if pre-existing cataract surgery was performed using measurements used when a ptosis was present. It is best for 2-3 months to have passed since any botulinum toxin A injections have been used in the periocular region.
This article in PDF format – “Through The Eagles Eye Vol. 3”
We have two convenient locations in Sydney. Our Mosman clinic on the Lower North Shore offers ground floor access, on-site parking, and excellent public transport links. Our Nepean clinic offers two hours of free on-site parking and easy access opposite Nepean Hospital. You can call us on (02) 7228 3900 (MOSMAN) or (02) 7228 3556 (NEPEAN) or arrange an appointment online through this website.

– Fellow of the Royal Australian and New Zealand College of Ophthalmologists (FRANZCO)
– Fellow of World College of Refractive Surgery and Visual Sciences (FWCRS)
– GradDipGraduate Diploma in Cataract and Refractive Surgery (University of Sydney)
– Master of Medicine (MMed, Ophthalmic Sciences, University of Sydney)
– Bachelor of Medicine and Surgery (MBBS, University of Tasmania)
Dr. Erica was a recipient of the 2022 ASCRS Foundation Resident Excellence Award. In 2019, she was awarded the RANZCO Filipic Greer Medal for overall excellence in performance at the RANZCO Ophthalmic Pathology examination. Most recently, she was awarded the Royal Australian and New Zealand College of Ophthalmologists (RANZCO) Trevalyn-Smith Travelling Scholarship to subsidize overseas study for Fellows.
As an accomplished researcher Dr. Erica’s work has been published widely in high quality medical journals, including the American Journal of Ophthalmology, the Journal of Cataract and Refractive Surgery, the European Journal of Ophthalmology and Clinical and Experimental Ophthalmology. Erica has also written a book chapter and has had the opportunity to present her research at various international and national conferences. Dr. Erica is appointed as a Clinical Lecturer in the Discipline of Ophthalmology at the University of Sydney, Save Sight Institute and regularly contributes to ongoing teaching in her area of subspeciality.